In 1941, a young Norwegian woman named Astrid L. suffered a traumatic brain injury after being struck by shrapnel during a bombing raid. When she regained consciousness and began speaking, her doctors were stunned: despite having never left Norway, she sounded unmistakably German. Her Norwegian had transformed into something listeners identified as French or German — a foreign accent acquired through brain damage alone.
This was the first documented case of Foreign Accent Syndrome, a rare and bizarre condition that has since been reported approximately 100 times worldwide. The syndrome transforms speech patterns so dramatically that listeners perceive a foreign accent, even though the patient has never lived in the associated country, studied the language, or had any exposure to the culture. An American might sound British, a Japanese speaker might sound Korean, or a Spaniard might sound Hungarian — all because of specific neurological changes.
The condition was first formally described in 1907 by French neurologist Pierre Marie, who documented a Parisian man who developed an Alsatian accent following a stroke. However, Astrid L.’s case, reported by Norwegian neurologist Georg Herman Monrad-Krohn in 1947, provided the first detailed clinical description and established FAS as a distinct neurological phenomenon. Monrad-Krohn’s patient had suffered damage to the left frontal lobe — the brain region controlling speech melody and rhythm — which altered her pronunciation, intonation, and syllable stress patterns. Frontiers in Psychology published a comprehensive review of this history in 2025.
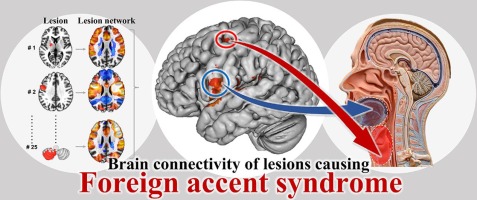
Modern neuroimaging has confirmed that FAS consistently involves damage to specific brain networks. A 2021 study in NeuroImage: Clinical used lesion network mapping to analyze 25 published cases of acquired neurogenic FAS. Researchers found that while the anatomical locations of lesions varied widely, at least 80% showed functional network overlap in the bilateral lower and middle portions of the precentral gyrus — the brain’s larynx motor cortex responsible for phonation, vowel production, and pitch accent. The middle portion specifically controls the muscles used for speaking and determines speech melody. The journal NeuroImage: Clinical published these findings in 2021.
This neurological specificity explains why FAS produces consistent acoustic changes. Patients typically alter their vowel pronunciation, substituting sounds like “ball” with “pall.” They inject filler sounds such as “uh” more frequently, distort multisyllabic words, and change their tongue placement during speech. These motor control changes alter the rhythm and prosody of speech — the musical qualities that listeners use to identify accents — without changing the underlying language or grammar. WebMD explained these speech changes in its 2024 medical review.
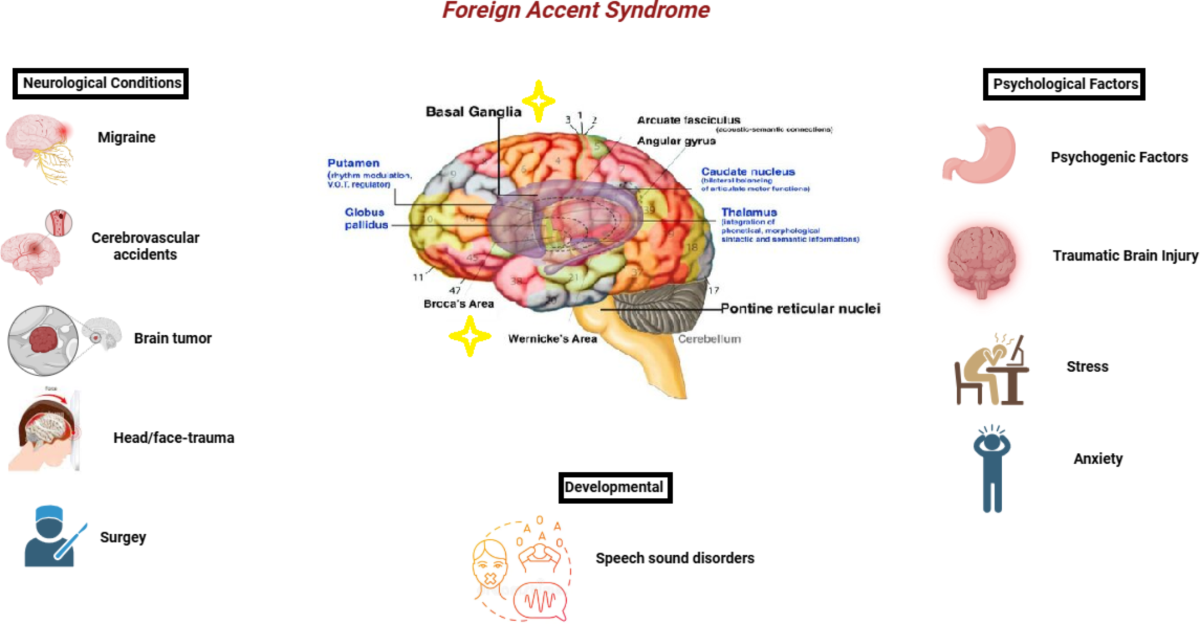
Not all cases stem from structural brain damage. A 2019 study analyzing 112 FAS cases found that approximately 70% were caused by stroke, with traumatic brain injury, brain tumors, and multiple sclerosis accounting for most others. However, Cleveland Clinic researchers have identified “functional FAS” cases where no structural lesion appears on MRI scans. These cases may involve abnormal brain activity organization or connections to functional neurological symptom disorder — formerly called conversion disorder — where psychological distress manifests as physical symptoms. Functional FAS has been associated with schizophrenia, bipolar disorder, and severe migraines. The Cleveland Clinic published these findings in 2023.
The psychiatric dimensions of FAS remain poorly understood. Research in the Indian Journal of Basic and Applied Medical Research in 2025 documented cases where FAS emerged without any detectable brain injury, suggesting psychogenic origins. One case involved a patient who developed a foreign accent during a psychotic episode, with the accent resolving when psychiatric symptoms were treated. The relationship between FAS and mental health conditions requires further investigation, complicated by the syndrome’s rarity.
Perhaps most fascinating are “developmental” cases where individuals report having a foreign accent since childhood without any brain injury. A study by researchers at Barcelonaβeta Brain Research Center examined two adult males who claimed to have had foreign accents since adolescence. While naive listeners couldn’t confirm foreign accents, detailed linguistic analysis revealed prosodic and segmental errors similar to acquired FAS cases. Brain imaging showed altered white matter microstructure in speech and emotion regulation networks, suggesting subtle developmental differences in brain organization rather than acquired damage. The Barcelonaβeta Brain Research Center published these findings.
Treatment options remain limited. Speech-language therapy can help patients manage articulation and prosody, teaching them to consciously control lip and jaw movements. However, the underlying neurological changes often persist. In stroke-related cases, approximately 20% of patients see their accents return to normal, while 40% of those with functional FAS experience symptom resolution. For many, the foreign accent becomes permanent, requiring psychological counseling to help patients adjust to their altered identity and social interactions. WebMD reported these statistics in its 2024 review.
The social consequences can be devastating. Patients report being accused of faking their accents, facing discrimination, or losing their sense of cultural identity. One patient described feeling like a stranger in her own country, unable to convince others that her accent was involuntary. The condition reveals how fundamentally speech connects to identity — when the accent changes, the person feels alienated from their own self-image.
Foreign Accent Syndrome demonstrates that accent — something we assume reflects cultural background, education, or personal choice — can be as mechanically determined as walking or breathing. The melody of our speech emerges from specific neural circuits controlling the larynx, tongue, and breath. When injury disrupts these circuits, the acoustic output changes, and listeners perceive a different identity. The syndrome forces us to confront uncomfortable questions about how much of our perceived identity is rooted in neural machinery that can be damaged, altered, or broken without our consent.
Bibliography
Barcelonaβeta Brain Research Center. (n.d.). Mild developmental foreign accent syndrome and psychiatric comorbidity: Altered white matter integrity in speech and emotion regulation networks. https://www.barcelonabeta.org/en/mild-developmental-foreign-accent-syndrome-and-psychiatric-comorbidity-altered-white-matter
Cleveland Clinic. (2023). Foreign accent syndrome. https://my.clevelandclinic.org/health/diseases/25242-foreign-accent-syndrome-fas
Frontiers in Psychology. (2025). Acquired language disorders beyond aphasia: Foreign accent syndrome as a neurological, speech, and psychiatric disorder. https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2025.1554104/full
Indian Journal of Basic and Applied Medical Research. (2025). Foreign accent syndrome: A language changing disorder. https://ijbpas.com/pdf/2025/August/MS_IJBPAS_2025_9272.pdf
NeuroImage: Clinical. (2021). Neural mechanisms of foreign accent syndrome: Lesion and network analysis. https://www.sciencedirect.com/science/article/pii/S2213158221002047