Imagine waking up tomorrow, looking at your spouse of 20 years, and feeling absolutely certain — despite their familiar face — that this person is an impostor. Not a stranger who looks similar, but an exact duplicate who has somehow replaced the person you love. You can see they look identical. You know it sounds crazy. But the emotional connection is gone, and you know something is terribly wrong.
This is the terrifying reality for people suffering from Capgras syndrome, one of the most bizarre and perplexing psychological conditions in neuroscience. First described in 1923 by French psychiatrist Joseph Capgras and his assistant Jean Reboul-Lachaux, the syndrome was initially called “l’illusion des sosies,” which essentially translates as the illusion of look-alikes. The original case involved a 53-year-old woman who believed her husband and daughter had been replaced by identical doubles, and the woman eventually began to to believe that everyone close to her was actually an imposter (Neuroscientifically Challenged, n.d.).
Capgras syndrome is surprisingly common in certain populations. Studies show it affects approximately 3% of hospitalized patients with psychosis and appears in roughly one in ten patients hospitalized for a first psychotic episode (National Center for Biotechnology Information, 2023). While historically associated with schizophrenia, researchers now recognize it frequently accompanies neurodegenerative diseases like Alzheimer’s, Lewy body dementia, and Parkinson’s disease (Cureus, 2024).
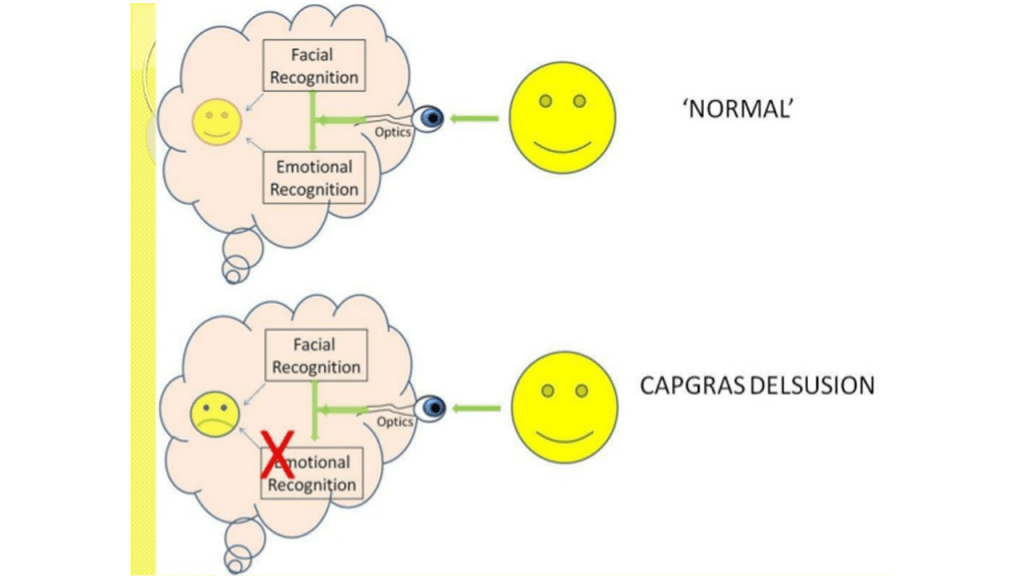
What makes Capgras syndrome particularly fascinating to neuroscientists is what it reveals about how we recognize the people we love. Most of us assume recognizing a spouse or parent is simple — you see their face, you know who they are. But the brain actually processes familiar faces through two distinct pathways working in tandem.
The first pathway handles conscious recognition — the “that’s my wife” identification. The second pathway, running from the temporal cortex to the limbic system (including the amygdala), generates the warm, familiar emotional response we feel when seeing loved ones (National Center for Biotechnology Information, 2023). In Capgras patients, the first pathway remains intact. They can still identify faces perfectly. But the second pathway — the emotional connection — is disrupted.
This creates a bizarre dissociation. The patient sees their husband’s face, recognizes it as their husband, but feels nothing. No warmth. No familiarity. Just the same emotional blankness they’d feel looking at a stranger on the subway. As one neuroscience blog explains, “Capgras delusion is sometimes described as the ‘mirror-image’ of prosopagnosia” — the condition where patients cannot recognize faces but still feel emotional responses to them (Neuroscientifically Challenged, n.d.).
Scientists have confirmed this using skin conductance response (SCR) testing, which measures subtle changes in perspiration indicating emotional arousal. When prosopagnosia patients see familiar faces, their SCR increases even though they cannot identify the person. Capgras patients show the opposite pattern — they can identify the face, but their SCR stays flat, as if looking at a stranger (Neuroscientifically Challenged, n.d.).
Harvard Medical School researchers mapped the brain lesions causing these delusions in a landmark study published in the journal Brain. They found that lesions in 17 Capgras patients were all functionally connected to the retrosplenial cortex — a region involved in perceiving familiarity — and most were also connected to the right ventral frontal cortex, which helps evaluate beliefs (Harvard Gazette, 2016). “With a lesion in exactly the right place, you can disrupt the brain’s familiarity detector and reality monitor simultaneously, resulting in bizarre delusions,” said Michael Fox, director of the Laboratory for Brain Network Imaging and Modulation (Harvard Gazette, 2016).
But why the impostor explanation? Why don’t patients simply think, “Something is wrong with my emotions”? Researchers believe it involves damage to frontal brain regions responsible for rational thought and belief evaluation. When confronted with the disturbing lack of emotion toward a loved one, the brain constructs the impostor narrative as an explanation — a way to resolve the cognitive dissonance (Neuroscientifically Challenged, n.d.).
The consequences can be devastating. Capgras patients may become hostile or violent toward the “impostor.” A 2004 review found homicide occurred in 6% of functional cases, with male patients showing higher violence risk (Cureus, 2024). One case study described a 46-year-old woman who threatened her husband with a knife and believed her daughters had been replaced by clowns (PMC, 2022).
Treatment remains challenging. Antipsychotic medications like quetiapine, olanzapine, and risperidone are the mainstay, with some evidence supporting antidepressants like mirtazapine (Archives of Medicine and Health Sciences, 2021; PMC, 2012). When depression underlies the syndrome, prognosis is better than when it accompanies schizophrenia (PMC, 2012). Caregivers are often advised to communicate from outside the patient’s line of sight, using voice recognition rather than face-to-face interaction, since auditory recognition pathways often remain intact (National Center for Biotechnology Information, 2023).
Bibliography